Lab 9 (ƒ 10) - Cranial Nerve Nuclei and Brain Stem Circulation
Cranial Nerve IV-Trochlear Nerve
The trochlear (IV) nerve is entirely motor and innervates the superior oblique muscle of the eye.
The trochlear nuclei can be visualized as the skull caps of two kissing elephants (see figure).
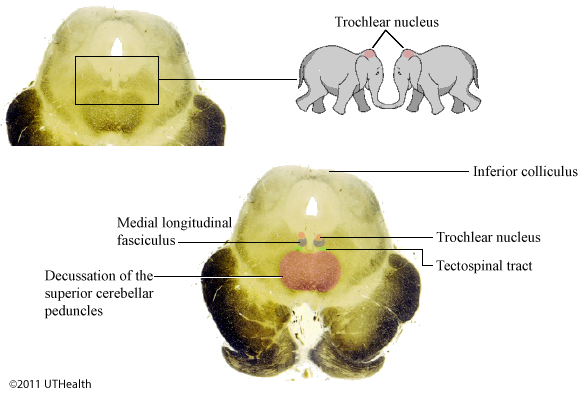 The trochlear nucleus axons pass posteriorly, decussate and exit the brain stem just caudal to the inferior colliculus. This is the only cranial nerve to leave the posterior aspect of the brain. They innervate the superior oblique muscle of the eye. Contraction of this muscle serves to intort the eye (roll the eye nasally) when abducted and depress the eye when adducted.
The trochlear nucleus axons pass posteriorly, decussate and exit the brain stem just caudal to the inferior colliculus. This is the only cranial nerve to leave the posterior aspect of the brain. They innervate the superior oblique muscle of the eye. Contraction of this muscle serves to intort the eye (roll the eye nasally) when abducted and depress the eye when adducted.
Damage to the trochlear motor neuron results in disorders that are difficult to detect. Patients may complain of vertical diplopia (double image) when walking down stairs or reading (attempted downward gaze) and may exhibit a slight convergent strabismus (abnormal position of the eye when attempting to gaze straight ahead).
The trochlear nucleus, like the other extraocular motor nuclei, receives inputs from a number of sources. Conjugate movements of the eye may be induced volitionally or reflexively in response to visual, vestibular or auditory stimuli. The extraocular motor nuclei receive
- Input from the other extraocular motor nuclei to coordinate muscle action;
- Indirect, supranuclear input from the frontal lobe for volitional saccades and from the parieto-temporal cortical areas for smooth pursuit;
- Input from vestibular centers for movement in response to alterations in head posture; and
- Input from midbrain centers for movement in response to sudden lights and sounds.
Disturbances in voluntary conjugate eye movements result from lesions interrupting the internal capsule. Impairment of voluntary eye movements may be accompanied by exaggerated fixation reflex. The patient may have difficulty in diverting his gaze from the object on which he is focusing.