Lab 9 (ƒ 10) - Cranial Nerve Nuclei and Brain Stem Circulation
Cranial Nerve VII - Facial Nerve
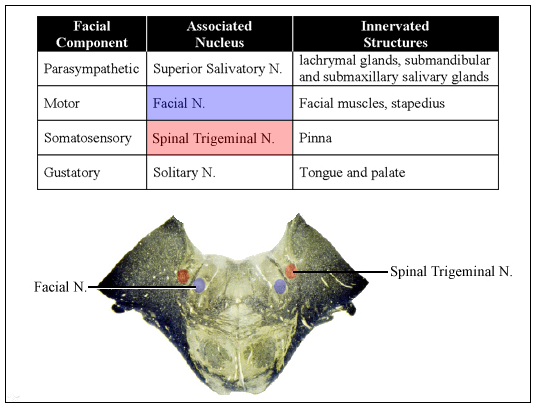
The components of the Facial (VII) Nerve include
- The motor fibers of the facial nucleus form the large facial motor root and innervate the facial muscles.
- The somatosensory afferent fibers innervating the pinna (that end in spinal trigeminal nuclei).
- The gustatory afferent fibers innervating the tongue and palate (that end in solitary nucleus).
- The visceral efferent fibers from the superior salivatory nucleus (that end in autonomic ganglia) constitute the smaller nervus intermedius root of the facial nerve.
 The facial nucleus consists of the cells of origin for the brachial motor component of the facial nerve. The fibers innervate the superficial skeletal muscles of the face and scalp (mimetic musculature), the platysma, the stylohyoid, the posterior belly of the digastric muscle and the stapedius muscle of the middle ear. Lesion of the facial motor neurons will result in a complete facial paralysis of the muscles normally innervated. Ipsilateral to the site of lesion, the mouth droops and the patient cannot whistle, wink or close the eye or wrinkle the forehead.
The facial nucleus consists of the cells of origin for the brachial motor component of the facial nerve. The fibers innervate the superficial skeletal muscles of the face and scalp (mimetic musculature), the platysma, the stylohyoid, the posterior belly of the digastric muscle and the stapedius muscle of the middle ear. Lesion of the facial motor neurons will result in a complete facial paralysis of the muscles normally innervated. Ipsilateral to the site of lesion, the mouth droops and the patient cannot whistle, wink or close the eye or wrinkle the forehead.
The facial nucleus receives inputs from the spinal trigeminal nucleus, which mediate the corneal blink and other trigeminofacial reflexes. A branch of the facial nerve innervates the stapedius muscle of the middle ear that controls middle ear sound transmission. The facial motor neurons innervating the stapedius receive auditory information from the superior olivary complex.
Corticofugal fibers exert direct and indirect influence bilaterally on cell groups innervating upper facial muscles and predominantly contralaterally on cell groups innervating the lower face. Unilateral lesions of corticofugal fibers produce a marked weakness of muscles in the lower half of the face contralaterally (especially in the mouth region) while muscles of the upper facial region concerned with wrinkling the forehead, frowning and closing the eyes are not affected. Even in the presence of this type of voluntary facial paralysis, the muscles in the lower face will contract symmetrically while smiling or laughing in response to a genuine emotional stimulus.
Since there are two different types of supranuclear facial paresis, one concerned with voluntary facial movement and another involving involuntary, emotional facial expression, there are at least two different pathways involved in controlling the facial muscles. Portions of the basal ganglia and the thalamus may be involved in the supranuclear control of emotional facial expression, but the actual pathways mediating these emotional influences are unknown.
Parasympathetic fibers of the superior salivatory nucleus travel in the nervus intermedius of the facial (VII) nerve and end in autonomic ganglia. In turn, these ganglia innervate the lacrimal glands, and the submandibular and submaxillary salivary glands. Damage to these autonomic efferents impairs salivary and lacrimal (tear) secretions. Inputs from the trigeminal sensory nuclei initiate reflex tearing in response to irritation of the eye. Inputs from the solitary nucleus and spinal trigeminal nucleus cause increased salivation from stimulation of the oral cavity. Bilateral corticofugal and hypothalamic inputs cause lacrimation and salivation in response to emotional and cognitive stimuli.
Clinical Testing of Cranial Nerve VII:
- Ask patient to raise eyebrows and wrinkle forehead. Test eye opening strength: Ask patient to close eyes as tight as they can and you try to open them.
- Ask patient to show teeth, smile or frown, or puff out cheeks against resistance while observing for symmetry.
- Test for gustatory sensation: test anterior 2/3 of tongue for sweet with sugar water, sour with citric acid, and salty with saline.